How Drinking Alcohol Affects Your Body
Alcohol has been used for thousands of years for various purposes — in ceremonies, during celebrations, and as a social lubricant, among other uses. We know alcohol is a toxin in nature, and there have been many claims thrown around as far as its health benefits and detriments.
While we’ll touch on the fact that moderate alcohol use is fine in many circumstances, we can’t ignore the fact that alcohol is one of the most used and abused substances in the United States. It is the third leading cause of preventable death here, and, as far as substances, it is the number one killer next to tobacco, leading even over opiates.
Excessive drinking increases the risk of cardiovascular and liver disease, metabolic disturbances, nutritional deficiencies, cancers (i.e. mouth, stomach, colon, liver, breast, and pancreatic cancer), neurological disorders, and fetal abnormalities.
In contrast to excessive alcohol use, light to moderate drinking, especially of alcoholic beverages rich in polyphenols such as red wine, was reported to lower the risk of coronary heart disease, stroke, type 2 diabetes, cognitive decline, and osteoporosis. Drinking excessively use will hurt body recomposition and fat loss efforts through various mechanisms, but light to moderate drinking may not be as harmful as we may think (with some exceptions that we’ll get into).
Table of Contents
Definitions
You’ll be reading a lot of references to “moderate alcohol use” or “heavy/excessive alcohol use” as we go further, so I want to define the terms to help you make informed choices moving forward.
In scientific literature, moderate drinking is defined as 1 drink per night for women and 2 drinks per night for men. Heavy drinking for women is defined as more than 3 drinks in any given sitting or more than 8 drinks per week, and for men, that goes to more than 4 drinks in any given sitting or more than 15 drinks per week.
There is a third level, dubbed “high intensity drinking” in studies, which we won’t mention very much, but this is defined as eight or more drinks in a sitting for women and ten or more drinks in a sitting for men — this is commonly referred to as binge drinking.
How Alcohol Consumption Impacts Hormones and Physical Health
The general theme that we’re going to be seeing here is that drinking alcohol exhibits a U-shaped curve depending on the amount ingested. For a lot of these outcomes, specifically more health-related outcomes, low to moderate amounts of alcohol show no detrimental effects, whereas drinking heavily always exhibits negative effects.
Too Much Alcohol Affects Sleep
The first thing we’ll talk about is sleep since we know that poor sleep has a trickle-down effect on hurting pretty much every aspect of our health.
With moderate drinking, results are a bit mixed. I could compare many different randomized controlled trials here just so you can get a view of the diversity of the data, but I’ll give a quote from a 2013 review that claims to be the most comprehensive review on alcohol and sleep:
“The effects on rapid eye movement (REM) sleep in the first half of sleep appear to be dose related with low and moderate doses showing no clear trend on REM sleep in the first half of the night.” When looking at entire-night REM %, they say the majority of studies saw less total REM% in individuals who drink heavily but no clear trend in moderate drinking. In fact, slow-wave sleep was actually increased with moderate doses.”
However, we know sleep is invariably compromised with higher doses, again to quote the authors: “At high doses, total REM % was significantly reduced.”
They then go on to state that “the majority of studies, regardless of low, moderate, or heavy drinking, age, and gender, confirm an increase in slow wave sleep (SWS) in the first half of the night relative to baseline values without alcohol. The impact of alcohol on (increasing) SWS in the first half of the night appears to be more robust than the (reduction) effect on REM sleep and does not appear to be an epiphenomenon of REM sleep reduction.”
We also know that alcohol use prior to bed, even moderate, can worsen sleep apnea. If you already have sleep apnea or have risk factors (snoring, large neck, overweight, etc.), then it’s highly likely that even low amounts of drinking will hurt your sleep.

Metabolic Effects and Insulin Resistance Associated With Alcohol
Once again, we have a U-shaped curve in terms of the risk of metabolic syndrome/insulin resistance/type 2 diabetes.
From the authors of a review study: “Low or moderate alcohol consumption shows protective effects against type 2 diabetes in patients through enhanced peripheral insulin sensitivity. A 30% reduced risk of type 2 diabetes was observed in patients with moderate alcohol consumption.”
Excessive alcohol consumption, on the other hand, is an independent risk factor for the development of type 2 diabetes. In addition to its effects on peripheral tissues, such as adipose tissue and liver, where it induces insulin resistance, heavy alcohol consumption was also proposed to negatively impact pancreatic ß-cell function.
Alcohol’s Effects on the HPG Axis and Sex Hormones
Testosterone
With sex hormones, many of the studies we are looking at break things into looking at acute effects, meaning levels of hormones directly after drinking alcohol, and others are looking more at long-term effects. I’ll specify which is which as we go through this section. Let’s start with moderate drinking.
There’s a lot of acute data, but we’d be more interested in longer-term data here. One study in non-resistance-trained individuals had men consume 3 beers every night and women consume 2 beers every night for 3 weeks. Plasma testosterone levels decreased in men by 6.8% after 3 beers per night for 3 weeks but found no effect in women.
Takeaway for moderate drinking: It doesn’t seem that having a few drinks a week, or even one day where you’re drinking a little more than moderately will impact testosterone levels. Three beers every night saw a small decrease in testosterone in non-resistance-trained men, but this amount of alcohol is also more than moderate drinking.
As far as heavy drinking, researchers really like to push the envelope when it comes to this. Many studies looking at heavy drinking and testosterone use doses of 1.5 g/kg of ethanol, which would translate to around 8 drinks for a 180 lb individual. Unsurprisingly, all studies using these doses show a significant decrease.
It also seems that the decrease can only be seen in men while an increase is evident in women. The increase in testosterone in women that is seen across the board has to be thought about contextually; for a woman with PCOS, this could be very harmful and may exacerbate her androgenic symptoms.
Female Cycle Health and Hormones
Jensen et al., in a study on 430 healthy women aged 20–35 years who were trying to conceive for the first time, found that alcohol intake, even as few as five or fewer drinks per week, was associated with decreased fertility and potential cycle disruptions.
In another study, 50% of “social drinkers” (4–6 drinks/week) saw significantly increased estradiol and prolactin, and some had irregular menstrual cycles (control for lifestyle and exclusion criteria was strict enough for them to be healthy otherwise). Moderate drinking didn’t seem to affect progesterone.
Other studies mirror this, so if your client is struggling with cycle health issues, this is one of the main arguments against drinking even moderate amounts of alcohol in these cases. It goes without saying heavy alcohol consumption pushes the negative effects further.
HPA Axis, and Cortisol
This one’s fairly interesting and a little nuanced. Basically, a subset of individuals will get a rise in cortisol and HPA axis hormones with even low to moderate drinking, while others won’t.
Individuals who get a cortisol release and HPA axis response with low levels tend to be those with a family history of alcoholism and are more predisposed to alcoholism, one of the reasons being it simply makes them feel better.
When we have a significant amount of cortisol flowing through the system, this generally gives us energy and makes us feel good. These will be the folks who get super rambunctious and end up with tons of energy after drinking 1 or 2 drinks.
But with heavy drinking, alcohol consumption mimics chronic stress; at first, all parts of the HPA axis get elevated, and if the consumption goes on long enough, everything will fall below baseline.
HPT Axis and Thyroid
Studies were pretty scarce on moderate consumption and thyroid hormone. One study monitored groups who then reported their daily alcohol consumption.
Men, on average, consumed 2 drinks an evening, and women consumed 1. The trend was slightly lower free T4 levels with TSH and free T3 unchanged.
With heavy drinking, however, TSH levels are increased and thyroid levels decrease.
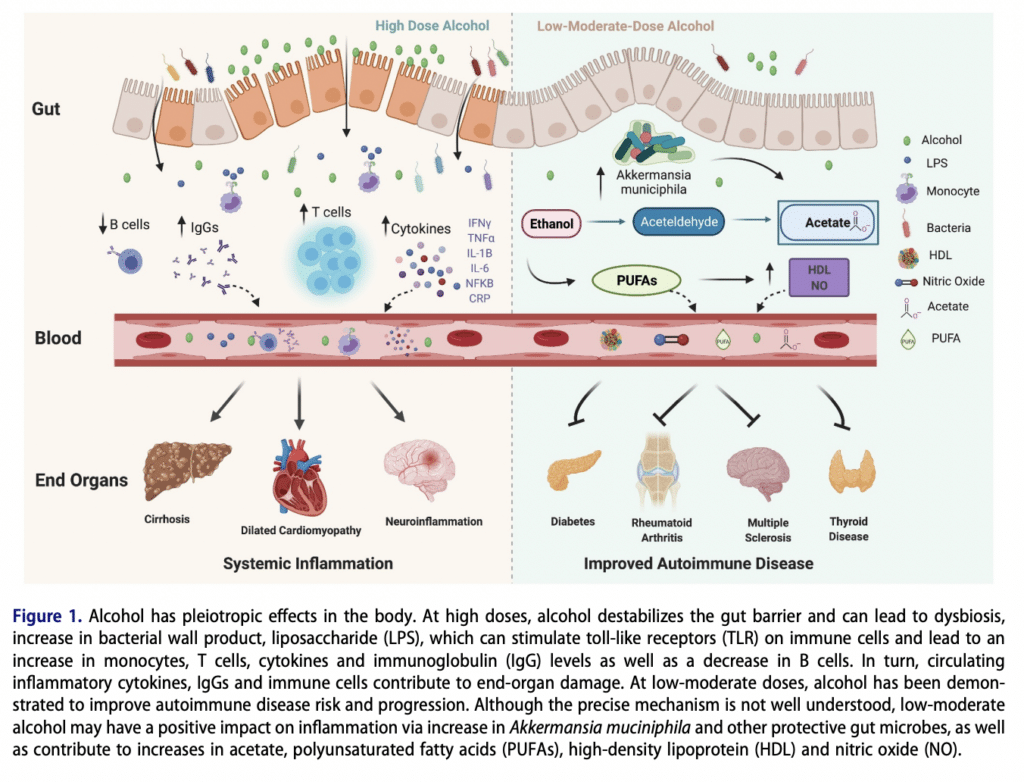
Alcohol Use and Gut and Autoimmune Diseases
A great review summarized both the effects of low-moderate and heavy doses of alcohol on multiple gut metrics as well as autoimmune diseases. The summary is that low-moderate doses do not affect gut permeability or gut dysbiosis in normal healthy individuals or even those with autoimmune diseases.
Low-moderate amounts of alcohol may actually have positive effects on gut bacteria. Recent evidence actually points toward alcohol’s protective effects in several autoimmune diseases, including autoimmune thyroid disease, autoimmune diabetes, systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), and multiple sclerosis (MS) in both human and animal studies.
Chronic heavy drinking, however, causes significant increases in gut permeability, gut-associated inflammation, dysbiosis, etc., also exacerbating autoimmune conditions.
It’s important to know that even small-moderate doses of alcohol may exacerbate pre-existing IBS; so it’s still one of the first things to eliminate when doing an elimination diet.
How to Go Out without Drinking Too Much Alcohol
As far as drinking moderately goes, if you’re just fitting 1–2 drinks into your daily macros every now and then, it would be safe to subtract those from either carbs or fat. If your client is an athlete, serious bodybuilder, or strength sport athlete, they probably won’t drink alcoholic beverages daily anyway, but if you have a lifestyle client who’s just looking to lose fat and wants to have a drink nightly or every other night, you can advise them to subtract from either fat or carbs. Keep in mind this is for a generally healthy individual, those with IBS may not do well with this level of moderate intake.
If you’re going for the fewest calories, think gin/vodka/whiskey (98-110 cals/drink) and soda water with lime or just neat, or go with a dry red or white wine (120-135 cals/drink). You can make some tasty low-calorie vodka and gin drinks with flavored soda water.
If you’re going to be going to an event or have some other circumstance where you’re going to be consuming a heavier amount of alcohol, here’s a little guide:
If you don’t want to accelerate or induce de novo lipogenesis (the creation of fat from carbs) and, at the same time, get more bang for your calorie buck (drink less for more of a buzz), I would go in with at least slightly depleted liver glycogen levels as well as on an empty stomach. This would mean eating light during the day; mostly protein and veggies and some fats.
Heavier alcohol consumption induces oxidative stress, and nicotinic acid (niacin or nicotinamide riboside) and zinc play large roles in alcohol metabolism. Therefore, a decent cocktail prior to a night of heavier drinking would be vitamin C, NAC or glutathione, zinc, and nicotinamide riboside or niacin; NR would be better than niacin. Studies show that people who had higher dietary nicotinic acid and zinc content had milder hangovers.
There is also a newer product on the market called Z-Biotics, which is a probiotic drink that specifically metabolizes excess acetaldehyde, preventing it from reaching the bloodstream and causing a worse hangover. Anecdotally, many people swear by this product to lessen or eliminate hangovers if taken before drinking.
After the first drink or two, you probably want to have a little food to hedge against getting too drunk too fast (or you can just stop drinking when you feel it). Ideally, you don’t want to eat a huge meal; the old adage of “eating to absorb alcohol” is not true.
The liver has to process the alcohol as well as whatever you eat, so if you over-indulge on food, depending on what you’re consuming, you could stress out your liver even more.
Be careful! After a few drinks and a buzz, you can easily stop paying as much attention to how much alcohol you’re consuming, and if your body is low on food, you can go from buzzed to drunk quite fast without realizing it.
Conclusion on the Effects of Alcohol on the Body
The TL;DR of this whole thing is that basically, moderate drinking (2 drinks a night for men, 1 for women) doesn’t seem to hurt much of physiology. The exceptions are potential sex hormone and cycle dysregulation for females, cortisol irregularities in those with a family history of alcoholism, and potential sleep disruption depending on the individual. There may be potential benefits with it for cardiovascular outcomes, insulin resistance, and autoimmune disease.
Since studies report averages, however, and people are individuals, I’d highly recommend assessing these things individually. These also don’t speak much to how these people feel on a daily basis or their quality of life; it could be that moderate drinking may cause a bit of fatigue if sleep is impaired. So the main take-home is to assess how YOU feel and how it affects your labwork, but if you fall into the “average,” moderate drinking is probably okay.
References
Cederbaum AI. Alcohol metabolism. Clin Liver Dis. 2012 Nov;16(4):667-85. doi: 10.1016/j.cld.2012.08.002. PMID: 23101976; PMCID: PMC3484320.
David F. Wilson, Franz M. Matschinsky. Ethanol metabolism: The good, the bad, and the ugly. Medical Hypotheses, Volume 140, 2020, 109638, ISSN 0306-9877, https://doi.org/10.1016/j.mehy.2020.109638.
Röjdmark S, Calissendorff J, Brismar K. Alcohol ingestion decreases both diurnal and nocturnal secretion of leptin in healthy individuals. Clin Endocrinol (Oxf). 2001 Nov;55(5):639-47. doi: 10.1046/j.1365-2265.2001.01401.x. PMID: 11894976.
Calissendorff, J., Danielsson, O., Brismar, K., & Röjdmark, S. (2005). Inhibitory effect of alcohol on ghrelin secretion in normal man, European Journal of Endocrinology eur j endocrinol, 152(5), 743-747. Retrieved Nov 21, 2021
Rachdaoui N, Sarkar DK. Effects of alcohol on the endocrine system. Endocrinol Metab Clin North Am. 2013 Sep;42(3):593-615. doi: 10.1016/j.ecl.2013.05.008. PMID: 24011889; PMCID: PMC3767933.
Health risks and benefits of alcohol consumption. Alcohol Res Health. 2000;24(1):5-11. PMID: 11199274; PMCID: PMC6713002.
Levitt DE, Idemudia NO, Cregar CM, Duplanty AA, Hill DW, Vingren JL. Alcohol After Resistance Exercise Does Not Affect Muscle Power Recovery. J Strength Cond Res. 2020 Jul;34(7):1938-1944. doi: 10.1519/JSC.0000000000002455. PMID: 29385007.
Lakićević N. The Effects of Alcohol Consumption on Recovery Following Resistance Exercise: A Systematic Review. J Funct Morphol Kinesiol. 2019 Jun 26;4(3):41. doi: 10.3390/jfmk4030041. PMID: 33467356; PMCID: PMC7739274.
El-Sayed MS, Ali N, El-Sayed Ali Z. Interaction between alcohol and exercise: physiological and haematological implications. Sports Med. 2005;35(3):257-69. doi: 10.2165/00007256-200535030-00005. PMID: 15730339.
Duplanty, Anthony A.1,2,3; Budnar, Ronald G.1; Luk, Hui Y.1,2; Levitt, Danielle E.1,2; Hill, David W.1; McFarlin, Brian K.1,2; Huggett, Duane B.2; Vingren, Jakob L.1,2 Effect of Acute Alcohol Ingestion on Resistance Exercise–Induced mTORC1 Signaling in Human Muscle, Journal of Strength and Conditioning Research: January 2017 – Volume 31 – Issue 1 – p 54-61
doi: 10.1519/JSC.0000000000001468
Bianco, A., Thomas, E., Pomara, F. et al. Alcohol consumption and hormonal alterations related to muscle hypertrophy: a review. Nutr Metab (Lond) 11, 26 (2014). https://doi.org/10.1186/1743-7075-11-26’
Sarkola T, Eriksson CJ. Testosterone increases in men after a low dose of alcohol. Alcohol Clin Exp Res. 2003 Apr;27(4):682-5. doi: 10.1097/01.ALC.0000060526.43976.68. PMID: 12711931.
Engen PA, Green SJ, Voigt RM, Forsyth CB, Keshavarzian A. The Gastrointestinal Microbiome: Alcohol Effects on the Composition of Intestinal Microbiota. Alcohol Res. 2015;37(2):223-36. PMID: 26695747; PMCID: PMC4590619.
Blaine Caslin, Kailey Mohler, Shreya Thiagarajan & Esther Melamed (2021)
Alcohol as friend or foe in autoimmune diseases: a role for gut microbiome?, Gut Microbes, 13:1, 1916278, DOI: 10.1080/19490976.2021.1916278
Caruana M, Cauchi R, Vassallo N. Putative Role of Red Wine Polyphenols against Brain Pathology in Alzheimer’s and Parkinson’s Disease. Front Nutr. 2016 Aug 12;3:31. doi: 10.3389/fnut.2016.00031. PMID: 27570766; PMCID: PMC4981604.
Richard EL, Kritz-Silverstein D, Laughlin GA, Fung TT, Barrett-Connor E, McEvoy LK. Alcohol Intake and Cognitively Healthy Longevity in Community-Dwelling Adults: The Rancho Bernardo Study. J Alzheimers Dis. 2017;59(3):803-814. doi: 10.3233/JAD-161153. PMID: 28671111; PMCID: PMC5939941.
Brust JC. Ethanol and cognition: indirect effects, neurotoxicity and neuroprotection: a review. Int J Environ Res Public Health. 2010 Apr;7(4):1540-57. doi: 10.3390/ijerph7041540. Epub 2010 Apr 4. PMID: 20617045; PMCID: PMC2872345.
Lundgaard, I., Wang, W., Eberhardt, A. et al. Beneficial effects of low alcohol exposure, but adverse effects of high alcohol intake on glymphatic function. Sci Rep 8, 2246 (2018). https://doi.org/10.1038/s41598-018-20424-y
Wang JJ, Tung TH, Yin WH, Huang CM, Jen HL, Wei J, Young MS. Effects of moderate alcohol consumption on inflammatory biomarkers. Acta Cardiol. 2008 Feb;63(1):65-72. doi: 10.2143/AC.63.1.2025334. PMID: 18372583.
Stote KS, Tracy RP, Taylor PR, Baer DJ. The effect of moderate alcohol consumption on biomarkers of inflammation and hemostatic factors in postmenopausal women. Eur J Clin Nutr. 2016 Apr;70(4):470-4. doi: 10.1038/ejcn.2015.182. Epub 2015 Nov 11. PMID: 26554758.
Pai JK, Hankinson SE, Thadhani R, Rifai N, Pischon T, Rimm EB. Moderate alcohol consumption and lower levels of inflammatory markers in US men and women. Atherosclerosis. 2006 May;186(1):113-20. doi: 10.1016/j.atherosclerosis.2005.06.037. Epub 2005 Aug 1. PMID: 16055129.
Steiner JL, Crowell KT, Lang CH. Impact of Alcohol on Glycemic Control and Insulin Action. Biomolecules. 2015 Sep 29;5(4):2223-46. doi: 10.3390/biom5042223. PMID: 26426068; PMCID: PMC4693236.
Barve S, Chen SY, Kirpich I, Watson WH, Mcclain C. Development, Prevention, and Treatment of Alcohol-Induced Organ Injury: The Role of Nutrition. Alcohol Res. 2017;38(2):289-302. PMID: 28988580; PMCID: PMC5513692.
Scott DM, Taylor RE. Health-related effects of genetic variations of alcohol-metabolizing enzymes in African Americans. Alcohol Res Health. 2007;30(1):18-21. PMID: 17718396; PMCID: PMC3860436.
Forsyth CB, Voigt RM, Burgess HJ, Swanson GR, Keshavarzian A. Circadian rhythms, alcohol and gut interactions. Alcohol. 2015 Jun;49(4):389-98. doi: 10.1016/j.alcohol.2014.07.021. Epub 2014 Nov 14. PMID: 25499101; PMCID: PMC4431951.
Kang, H., Park, YK. & Lee, JY. Nicotinamide riboside, an NAD+ precursor, attenuates inflammation and oxidative stress by activating sirtuin 1 in alcohol-stimulated macrophages. Lab Invest 101, 1225–1237 (2021). https://doi.org/10.1038/s41374-021-00599-1
Roth MJ, Baer DJ, Albert PS, Castonguay TW, Dorgan JF, Dawsey SM, Brown ED, Hartman TJ, Campbell WS, Giffen CA, Judd JT, Taylor PR. Relationship between serum leptin levels and alcohol consumption in a controlled feeding and alcohol ingestion study. J Natl Cancer Inst. 2003 Nov 19;95(22):1722-5. doi: 10.1093/jnci/djg090. PMID: 14625264.
Suter PM, Jéquier E, Schutz Y. Effect of ethanol on energy expenditure. Am J Physiol. 1994 Apr;266(4 Pt 2):R1204-12. doi: 10.1152/ajpregu.1994.266.4.R1204. PMID: 8184963.
Blaine SK, Milivojevic V, Fox H, Sinha R. Alcohol Effects on Stress Pathways: Impact on Craving and Relapse Risk. Can J Psychiatry. 2016 Mar;61(3):145-53. doi: 10.1177/0706743716632512. Epub 2016 Feb 9. PMID: 27254089; PMCID: PMC4813419.
Feige, B., Gann, H., Brueck, R., Hornyak, M., Litsch, S., Hohagen, F. and Riemann, D. (2006), Effects of Alcohol on Polysomnographically Recorded Sleep in Healthy Subjects. Alcoholism: Clinical and Experimental Research, 30: 1527-1537. https://doi.org/10.1111/j.1530-0277.2006.00184.x
Ebrahim, I.O., Shapiro, C.M., Williams, A.J. and Fenwick, P.B. (2013), Alcohol and Sleep I: Effects on Normal Sleep. Alcohol Clin Exp Res, 37: 539`-549. https://doi.org/10.1111/acer.12006
Park SY, Oh MK, Lee BS, Kim HG, Lee WJ, Lee JH, Lim JT, Kim JY. The Effects of Alcohol on Quality of Sleep. Korean J Fam Med. 2015 Nov;36(6):294-9. doi: 10.4082/kjfm.2015.36.6.294. Epub 2015 Nov 20. PMID: 26634095; PMCID: PMC4666864.
Scanlan MF, Roebuck T, Little PJ, Redman JR, Naughton MT. Effect of moderate alcohol upon obstructive sleep apnoea. Eur Respir J. 2000 Nov;16(5):909-13. doi: 10.1183/09031936.00.16590900. PMID: 11153591.
Sierksma A, Sarkola T, Eriksson CJ, van der Gaag MS, Grobbee DE, Hendriks HF. Effect of moderate alcohol consumption on plasma dehydroepiandrosterone sulfate, testosterone, and estradiol levels in middle-aged men and postmenopausal women: a diet-controlled intervention study. Alcohol Clin Exp Res. 2004 May;28(5):780-5. doi: 10.1097/01.alc.0000125356.70824.81. PMID: 15166654.
Parr EB, Camera DM, Areta JL, Burke LM, Phillips SM, Hawley JA, Coffey VG. Alcohol ingestion impairs maximal post-exercise rates of myofibrillar protein synthesis following a single bout of concurrent training. PLoS One. 2014 Feb 12;9(2):e88384. doi: 10.1371/journal.pone.0088384. PMID: 24533082; PMCID: PMC3922864.
Verster JC, Vermeulen SA, Loo AJAEV, Balikji S, Kraneveld AD, Garssen J, Scholey A. Dietary Nutrient Intake, Alcohol Metabolism, and Hangover Severity. J Clin Med. 2019 Aug 27;8(9):1316. doi: 10.3390/jcm8091316. PMID: 31461972; PMCID: PMC6780234.
Elizabeth R. De Oliveira e Silva , MD , David Foster , PhD , Monnie McGee Harper , PhD , Cynthia E. Seidman , MS, RD , Jonathan D. Smith , PhD , Jan L. Breslow , MD , and Eliot A. Brinton , MD. Alcohol Consumption Raises HDL Cholesterol Levels by Increasing the Transport Rate of Apolipoproteins A-I and A-II. 7 Nov 2000. https://doi.org/10.1161/01.CIR.102.19.2347Circulation. 2000;102:2347–2352
Huang S, Li J, Shearer GC, Lichtenstein AH, Zheng X, Wu Y, Jin C, Wu S, Gao X. Longitudinal study of alcohol consumption and HDL concentrations: a community-based study. Am J Clin Nutr. 2017 Apr;105(4):905-912. doi: 10.3945/ajcn.116.144832. Epub 2017 Mar 1. PMID: 28251934; PMCID: PMC5366050.